Active Aerosol Mitigation System for Healthcare Workers
Portable, low-cost active aerosol mitigation system for high-risk respiratory therapies. 99.0% peak aerosol reduction during HFNC nebulization without compromising drug delivery. Deployed in 1,100+ clinical cases. Peer-reviewed in Emerg. Care Med. (2025).
Overview
Co-led the development and validation of a portable active aerosol mitigation system to protect healthcare workers during high-risk respiratory therapies. Took the project from engineering design through clinical validation and peer-reviewed publication (Emergency Care and Medicine, 2025), in a collaboration between ASU’s Biodesign Institute and Mayo Clinic.
Problem
Aerosol-generating procedures like nebulization with HFNC or non-invasive ventilation expose healthcare workers to infectious airborne particles (under 10 µm) capable of transmitting pathogens like SARS-CoV-2, influenza, and measles. Existing solutions like surgical masks and containment boxes leave most fugitive aerosols unmitigated, and hospital HVAC upgrades aren’t a viable point-of-care fix. I set out to build a portable, low-cost system that solves this at the source.
Approach
I engineered and tested two active mitigation systems:
- An aerosol barrier mask combining a fitted silicone oronasal mask, biofilter (0.2 µm pore, 99.99%+ bacterial/viral efficiency), and a battery-powered fan for HFNC.
- A containment box with the same fan and biofilter assembly for NIV.
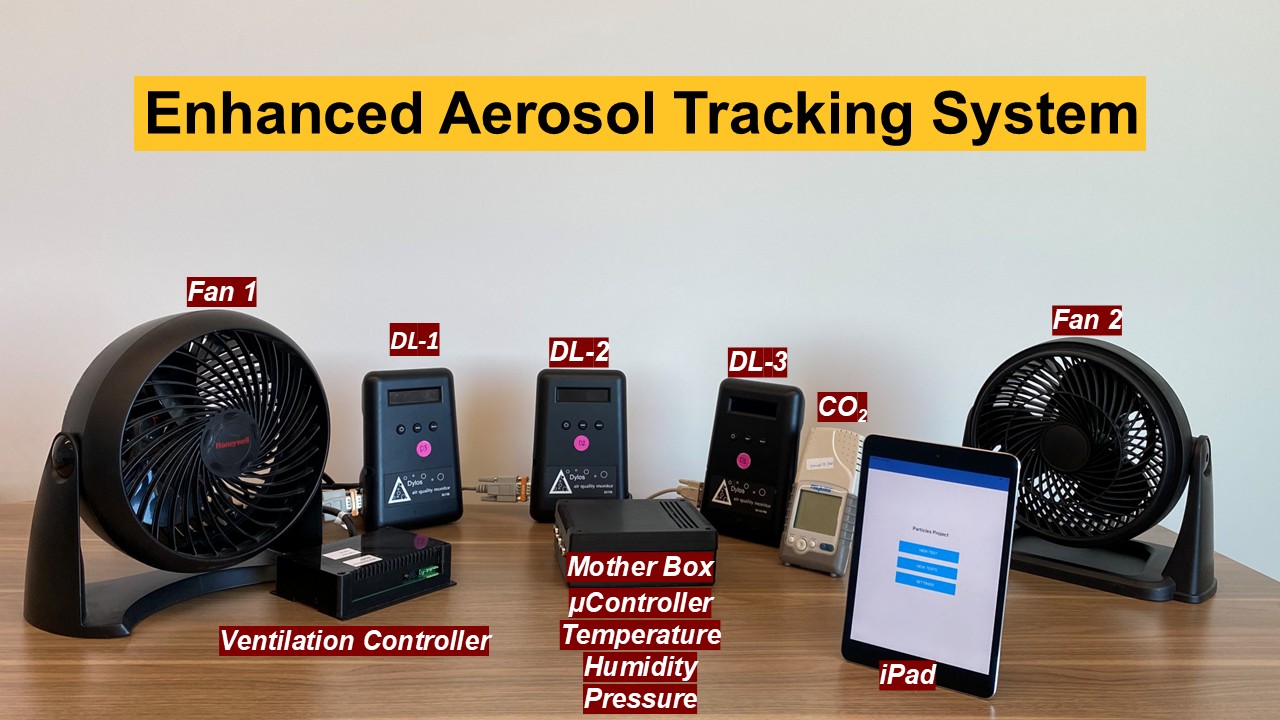
I designed the experimental framework to benchmark both against passive controls in a simulated airborne infection isolation room, deploying redundant aerosol sensors (Dylos DC1100 Pro and MET ONE HHPC2+) at 3, 6, and 13 ft. I quantified mitigation efficacy through peak and area-under-curve analysis of aerosol concentration-time profiles, and independently validated that the active system didn’t compromise nebulized drug delivery across saline, albuterol, vancomycin, and amikacin.


Results
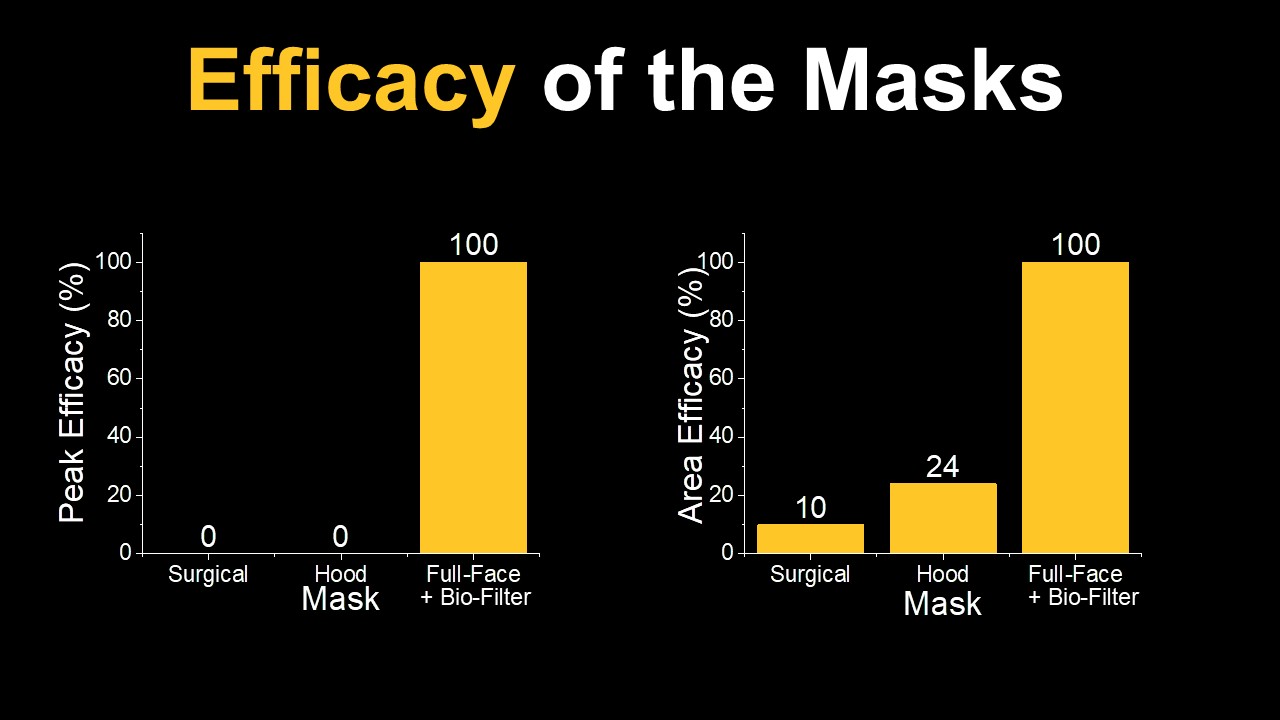
The active system dramatically outperformed existing approaches:
- 99.0% peak / 96.4% area aerosol reduction for HFNC + nebulization (vs. 35.9% / 7.6% with a surgical mask).
- 92.1% peak / 84.5% area reduction for NIV + nebulization (vs. 53.7% / 25.4% with the box alone).
- Drug delivery remained statistically unaffected (p > 0.1 across all four medications: saline, albuterol, vancomycin, amikacin).
- Applied through the Wells–Riley infection risk framework, the system reduces estimated infection probability to under 1% (HFNC) and 12% (NIV).
- The mask was deployed in over 1,100 clinical cases during the pandemic with positive frontline feedback: a real-world validation of the design.